Childhood Thyroid Cancer Treatment (PDQ®): Treatment - Health Professional Information [NCI]
This information is produced and provided by the National Cancer Institute (NCI). The information in this topic may have changed since it was written. For the most current information, contact the National Cancer Institute via the Internet web site at http://cancer.gov or call 1-800-4-CANCER.
Incidence
The annual incidence of thyroid cancers is 2.0 cases per 1 million people per year in children younger than 15 years, accounting for approximately 1.5% of all cancers in this age group.[1] Thyroid cancer incidence is higher in children aged 15 to 19 years (17.6 cases per 1 million people), and it accounts for approximately 8% of cancers arising in this older age group.[1,2] More thyroid carcinomas occur in females than in males.[3]
A retrospective review of the Surveillance, Epidemiology, and End Results (SEER) database from 1973 to 2011 identified 2,504 cases of papillary thyroid carcinoma in patients aged 20 years and younger.[2] The incidence of papillary thyroid carcinoma increased over this interval by roughly 2% each year. The trend toward larger tumors suggests that diagnostic scrutiny is not the only explanation for the observed results.[4]
An update from the SEER database for the period of 2007 to 2012 identified 1,723 pediatric patients with thyroid cancer.[5] The average age-adjusted incidence of pediatric thyroid cancer was 0.59 cases per 100,000 patients. When the incidence in females was compared with the incidence in males, the ratio of pediatric thyroid cancer was 4.4:1. The incidences of papillary, follicular variant, follicular, and medullary subtypes differ over the pediatric age range (refer to Figure 1).[5]
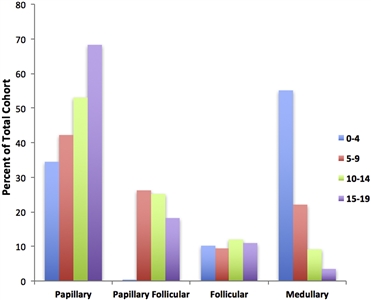
Figure 1. Incidence of pediatric thyroid carcinoma based on most frequent subtype per 100,000 as a percent of total cohort. Reprinted from International Journal of Pediatric Otorhinolaryngology, Volume 89, Sarah Dermody, Andrew Walls, Earl H. Harley Jr., Pediatric thyroid cancer: An update from the SEER database 2007-2012, Pages 121-126, Copyright (2016), with permission from Elsevier.
References:
- Horner MJ, Ries LA, Krapcho M, et al.: SEER Cancer Statistics Review, 1975-2006. Bethesda, Md: National Cancer Institute, 2009. Also available online. Last accessed September 28, 2017.
- Golpanian S, Perez EA, Tashiro J, et al.: Pediatric papillary thyroid carcinoma: outcomes and survival predictors in 2504 surgical patients. Pediatr Surg Int 32 (3): 201-8, 2016.
- Shapiro NL, Bhattacharyya N: Population-based outcomes for pediatric thyroid carcinoma. Laryngoscope 115 (2): 337-40, 2005.
- Vergamini LB, Frazier AL, Abrantes FL, et al.: Increase in the incidence of differentiated thyroid carcinoma in children, adolescents, and young adults: a population-based study. J Pediatr 164 (6): 1481-5, 2014.
- Dermody S, Walls A, Harley EH Jr: Pediatric thyroid cancer: An update from the SEER database 2007-2012. Int J Pediatr Otorhinolaryngol 89: 121-6, 2016.
Risk Factors
There is an excessive frequency of thyroid adenoma and carcinoma in patients who previously received radiation to the neck.[1,2] In the decade following the Chernobyl nuclear incident, there was a tenfold increase in the incidence of thyroid cancer compared with the previous and following decades.[3] In this group of patients with exposure to low-dose radiation, tumors commonly show a gain of chromosome band 7q11.[4]
When occurring in patients with the multiple endocrine neoplasia syndromes, thyroid cancer may be associated with the development of other types of malignant tumors. (Refer to the Multiple Endocrine Neoplasia [MEN] Syndromes and Carney Complex section of the PDQ summary on Unusual Cancers of Childhood Treatment for more information.)
References:
- Cotterill SJ, Pearce MS, Parker L: Thyroid cancer in children and young adults in the North of England. Is increasing incidence related to the Chernobyl accident? Eur J Cancer 37 (8): 1020-6, 2001.
- Kaplan MM, Garnick MB, Gelber R, et al.: Risk factors for thyroid abnormalities after neck irradiation for childhood cancer. Am J Med 74 (2): 272-80, 1983.
- Demidchik YE, Saenko VA, Yamashita S: Childhood thyroid cancer in Belarus, Russia, and Ukraine after Chernobyl and at present. Arq Bras Endocrinol Metabol 51 (5): 748-62, 2007.
- Hess J, Thomas G, Braselmann H, et al.: Gain of chromosome band 7q11 in papillary thyroid carcinomas of young patients is associated with exposure to low-dose irradiation. Proc Natl Acad Sci U S A 108 (23): 9595-600, 2011.
Histology
Tumors of the thyroid are classified as adenomas or carcinomas.[1,2,3] Adenomas are benign, well circumscribed and encapsulated nodules that may cause enlargement of all or part of the gland, which extends to both sides of the neck and can be quite large; some tumors may secrete hormones. Transformation to a malignant carcinoma may occur in some cells, which may grow and spread to lymph nodes in the neck or to the lungs. Approximately 20% of thyroid nodules in children are malignant.[1,4]
Various histologies account for the general diagnostic category of carcinoma of the thyroid; papillary and follicular carcinoma are often referred to as differentiated thyroid carcinoma:[5]
- Papillary carcinoma (60%-75%): Papillary carcinoma often has a multicentric origin and a very high rate of lymph node metastasis (70%-90%).[6] Metastases to the lungs occur in about 25% of cases. Papillary carcinoma generally has a benign course, with a 10-year survival rate of more than 95%.[7,8] Overall, long-term outcomes for children and adolescents with papillary thyroid cancer are excellent, with 2% cause-specific mortality at 40 years.[8]
- Follicular carcinoma (10%-20%): Follicular carcinoma is usually encapsulated and has a higher incidence of bone and lung metastases.[6] It may be sporadic or familial.[9] Follicular carcinoma also has a generally benign course, with a 10-year survival rate of more than 95%.[7]
- Medullary carcinoma (5%-10%): Medullary carcinoma is a form of thyroid carcinoma that originates from the calcitonin-secreting parafollicular C cells. It is usually familial.[9]
- Anaplastic carcinoma (<1%).
References:
- Dinauer C, Francis GL: Thyroid cancer in children. Endocrinol Metab Clin North Am 36 (3): 779-806, vii, 2007.
- Vasko V, Bauer AJ, Tuttle RM, et al.: Papillary and follicular thyroid cancers in children. Endocr Dev 10: 140-72, 2007.
- Halac I, Zimmerman D: Thyroid nodules and cancers in children. Endocrinol Metab Clin North Am 34 (3): 725-44, x, 2005.
- Francis GL, Waguespack SG, Bauer AJ, et al.: Management Guidelines for Children with Thyroid Nodules and Differentiated Thyroid Cancer. Thyroid 25 (7): 716-59, 2015.
- Kaplan MM, Garnick MB, Gelber R, et al.: Risk factors for thyroid abnormalities after neck irradiation for childhood cancer. Am J Med 74 (2): 272-80, 1983.
- Feinmesser R, Lubin E, Segal K, et al.: Carcinoma of the thyroid in children--a review. J Pediatr Endocrinol Metab 10 (6): 561-8, 1997 Nov-Dec.
- Hung W, Sarlis NJ: Current controversies in the management of pediatric patients with well-differentiated nonmedullary thyroid cancer: a review. Thyroid 12 (8): 683-702, 2002.
- Hay ID, Gonzalez-Losada T, Reinalda MS, et al.: Long-term outcome in 215 children and adolescents with papillary thyroid cancer treated during 1940 through 2008. World J Surg 34 (6): 1192-202, 2010.
- Skinner MA: Management of hereditary thyroid cancer in children. Surg Oncol 12 (2): 101-4, 2003.
Molecular Features and Tumor Characteristics
Studies have shown subtle differences between the genetic profiling of childhood differentiated thyroid carcinomas and that of adult tumors (refer to Table 1). In one study, a higher prevalence of RET/PTC rearrangements was reported in pediatric papillary thyroid carcinoma (45%-65% in children vs. 3%-34% in adults).[1]BRAF V600E mutations are seen in more than 50% of adults with papillary thyroid carcinoma;[2] although it likely occurs in a similar frequency in pediatric patients, studies have revealed a wide variation in frequency of this mutation.[1,2,3,4] In children, the correlation between the genomic alteration and stage or prognosis has not been well defined. While two studies failed to show a correlation,[3,4] one study that included 55 pediatric thyroid carcinoma cases demonstrated a significant correlation between the presence of a BRAF V600E mutation and an increased risk of recurrence.[5] Differentiated thyroid carcinoma has been associated with germline DICER1 mutations and it is considered part of the DICER1 syndrome.[6]
| Characteristic | Children and Adolescents (%) | Adults (%) |
|---|---|---|
| a Yamashita et al.,[7]Nikita et al.,[4]and Alzahrani et al.[5] | ||
| Gene rearrangements: | ||
| RET/PTC | 21-87 | 0-35 |
| NTRK 1 | 5-11 | 5-13 |
| AKAP9-BRAF | 11 | 1 |
| PAX8-PPARG | Unknown | 0-50 |
| Point mutations: | ||
| BRAF | 0-63 | 0-43 |
| RASfamily | 0-16 | 25-69 |
| GNAS | 0 | 11 |
| TP53 | 0-23 | 0-20 |
| TERT | 0 | 16 |
| Other: | ||
| Multicentric | 30-50 | 40-56 |
| Lymph node involvement | 30-90 | 5-55 |
| Extrathyroid extension | 24-51 | 16-46 |
| Vascular invasion | <31 | 14-37 |
| Distant metastases | 10-20 | 5-10 |
References:
- Ballester LY, Sarabia SF, Sayeed H, et al.: Integrating Molecular Testing in the Diagnosis and Management of Children with Thyroid Lesions. Pediatr Dev Pathol 19 (2): 94-100, 2016 Mar-Apr.
- Rivkees SA, Mazzaferri EL, Verburg FA, et al.: The treatment of differentiated thyroid cancer in children: emphasis on surgical approach and radioactive iodine therapy. Endocr Rev 32 (6): 798-826, 2011.
- Henke LE, Perkins SM, Pfeifer JD, et al.: BRAF V600E mutational status in pediatric thyroid cancer. Pediatr Blood Cancer 61 (7): 1168-72, 2014.
- Nikita ME, Jiang W, Cheng SM, et al.: Mutational Analysis in Pediatric Thyroid Cancer and Correlations with Age, Ethnicity, and Clinical Presentation. Thyroid 26 (2): 227-34, 2016.
- Alzahrani AS, Qasem E, Murugan AK, et al.: Uncommon TERT Promoter Mutations in Pediatric Thyroid Cancer. Thyroid 26 (2): 235-41, 2016.
- Slade I, Bacchelli C, Davies H, et al.: DICER1 syndrome: clarifying the diagnosis, clinical features and management implications of a pleiotropic tumour predisposition syndrome. J Med Genet 48 (4): 273-8, 2011.
- Yamashita S, Saenko V: Mechanisms of Disease: molecular genetics of childhood thyroid cancers. Nat Clin Pract Endocrinol Metab 3 (5): 422-9, 2007.
Clinical Presentation and Outcome
Patients with thyroid cancer usually present with a thyroid mass with or without painless cervical adenopathy.[1,2,3] On the basis of medical and family history and clinical constellation, the thyroid cancer may be part of a tumor predisposition syndrome such as multiple endocrine neoplasia or DICER1 syndrome.[4]
Younger age is associated with a more aggressive clinical presentation in differentiated thyroid carcinoma. Children have a higher proportion of nodal involvement (40%-90% in children vs. 20%-50% in adults) and lung metastases (20%-30% in children vs. 2% in adults) than do adults.[5,6] Larger tumor size (>1 cm), extrathyroidal extension, and multifocal disease are associated with increased risk of nodal metastases.[7] Likewise, when compared with pubertal adolescents, prepubertal children have a more aggressive presentation with a greater degree of extrathyroid extension, lymph node involvement, and lung metastases. However, outcome is similar in the prepubertal and adolescent groups.[8]
In well-differentiated thyroid cancer, male sex, large tumor size, and distant metastases have been found to have prognostic significance for early mortality; however, even patients in the highest risk group who have distant metastases had excellent survival at 90%.[9] A French registry analysis found similar outcomes in children and young adults who developed papillary thyroid carcinoma after previous radiation therapy compared with children and young adults who developed spontaneous papillary thyroid carcinoma; patients with previous thyroid irradiation for benign disease, however, presented with more invasive tumors and lymph node involvement.[10]
References:
- Thompson GB, Hay ID: Current strategies for surgical management and adjuvant treatment of childhood papillary thyroid carcinoma. World J Surg 28 (12): 1187-98, 2004.
- Rachmiel M, Charron M, Gupta A, et al.: Evidence-based review of treatment and follow up of pediatric patients with differentiated thyroid carcinoma. J Pediatr Endocrinol Metab 19 (12): 1377-93, 2006.
- Wada N, Sugino K, Mimura T, et al.: Treatment strategy of papillary thyroid carcinoma in children and adolescents: clinical significance of the initial nodal manifestation. Ann Surg Oncol 16 (12): 3442-9, 2009.
- Schultz KA, Yang J, Doros L, et al.: DICER1-pleuropulmonary blastoma familial tumor predisposition syndrome: a unique constellation of neoplastic conditions. Pathol Case Rev 19 (2): 90-100, 2014.
- Rivkees SA, Mazzaferri EL, Verburg FA, et al.: The treatment of differentiated thyroid cancer in children: emphasis on surgical approach and radioactive iodine therapy. Endocr Rev 32 (6): 798-826, 2011.
- Al-Qurayshi Z, Hauch A, Srivastav S, et al.: A National Perspective of the Risk, Presentation, and Outcomes of Pediatric Thyroid Cancer. JAMA Otolaryngol Head Neck Surg 142 (5): 472-8, 2016.
- Kim J, Sun Z, Adam MA, et al.: Predictors of nodal metastasis in pediatric differentiated thyroid cancer. J Pediatr Surg 52 (1): 120-123, 2017.
- Lazar L, Lebenthal Y, Steinmetz A, et al.: Differentiated thyroid carcinoma in pediatric patients: comparison of presentation and course between pre-pubertal children and adolescents. J Pediatr 154 (5): 708-14, 2009.
- Shayota BJ, Pawar SC, Chamberlain RS: MeSS: A novel prognostic scale specific for pediatric well-differentiated thyroid cancer: a population-based, SEER outcomes study. Surgery 154 (3): 429-35, 2013.
- Sassolas G, Hafdi-Nejjari Z, Casagranda L, et al.: Thyroid cancers in children, adolescents, and young adults with and without a history of childhood exposure to therapeutic radiation for other cancers. Thyroid 23 (7): 805-10, 2013.
Diagnostic Evaluation
Initial evaluation of a child or adolescent with a thyroid nodule includes the following:
- Ultrasound of the thyroid.
- Serum thyroid-stimulating hormone (TSH) level.
- Serum thyroglobulin level.
Tests of thyroid function are usually normal, but thyroglobulin can be elevated.
Fine-needle aspiration as an initial diagnostic approach is sensitive and useful. However, in doubtful cases, open biopsy or resection should be considered.[1,2,3,4] Open biopsy or resection may also be preferable for young children (refer to Table 2).
| Histology | Associated Chromosomal Abnormality | Presentation | Diagnosis | Treatment |
|---|---|---|---|---|
| EGF = epidermal growth factor; 131I = iodine I 131; MEN2 = multiple endocrine neoplasia type 2; TSH = thyroid-stimulating hormone. | ||||
| Differentiated thyroid carcinoma | RET/PTCmore common in children.BRAFV600E mutations occur with similar frequency in children and adults. Association with rare hereditary tumor syndromes:APC-associated polyposis,DICER1syndrome, Carney complex,PTENhamartoma tumor syndrome, Werner syndrome. | Thyroid mass. Prepubertal children more often with nodal and lung metastases. | Ultrasound, TSH, thyroglobulin. Fine needle or open biopsy. | Total or near-total thyroidectomy; 131I; thyroid hormone. In metastatic or recurrent disease, tyrosine kinase or EGF receptor inhibitors may be of benefit. |
| Medullary thyroid carcinoma | MEN2 | Aggressive. 50% with metastases at presentation. | In familial MEN2,RETtesting. | Aggressive surgical intervention. Prophylactic thyroidectomy is indicated in familial cases. |
References:
- Willgerodt H, Keller E, Bennek J, et al.: Diagnostic value of fine-needle aspiration biopsy of thyroid nodules in children and adolescents. J Pediatr Endocrinol Metab 19 (4): 507-15, 2006.
- Stevens C, Lee JK, Sadatsafavi M, et al.: Pediatric thyroid fine-needle aspiration cytology: a meta-analysis. J Pediatr Surg 44 (11): 2184-91, 2009.
- Bargren AE, Meyer-Rochow GY, Sywak MS, et al.: Diagnostic utility of fine-needle aspiration cytology in pediatric differentiated thyroid cancer. World J Surg 34 (6): 1254-60, 2010.
- Redlich A, Boxberger N, Kurt Werner S, et al.: Sensitivity of fine-needle biopsy in detecting pediatric differentiated thyroid carcinoma. Pediatr Blood Cancer 59 (2): 233-7, 2012.
Treatment of Papillary and Follicular Thyroid Carcinoma
Treatment options for papillary and follicular (differentiated) thyroid carcinoma may include the following:
- Surgery.
- Radioactive iodine ablation.
The management of differentiated thyroid cancer in children has been reviewed in detail.[1,2] In 2015, the American Thyroid Association (ATA) Task Force on Pediatric Thyroid Cancer published guidelines for the management of thyroid nodules and differentiated thyroid cancer in children and adolescents. These guidelines (summarized below) are based on scientific evidence and expert panel opinion, with a careful assessment of the level of evidence.[2]
- Preoperative evaluation.[2]
- A comprehensive ultrasound of all regions of the neck using a high-resolution probe and Doppler technique should be obtained by an experienced ultrasonographer. A complete ultrasound examination should be performed before surgery.
- The addition of cross-sectional imaging (contrast-enhanced computed tomography [CT] or magnetic resonance imaging) should be considered when there is concern about invasion of the aerodigestive tract. Importantly, if iodinated contrast agents are used, further evaluation and treatment with radioactive iodine may need to be delayed for 2 to 3 months until total body iodine burden decreases.
- Chest imaging (x-ray or CT) may be considered for patients with substantial cervical lymph node disease.
- Thyroid nuclear scintigraphy should be pursued only if the patient presents with a suppressed thyroid-stimulating hormone (TSH).
- The routine use of bone scan or fluorine F 18-fludeoxyglucose positron emission tomography (PET) is not recommended.
- Surgery.[2]
Pediatric thyroid surgery should ideally be performed by a surgeon who performs at least 30 or more cervical endocrine procedures annually in a hospital with the full spectrum of pediatric specialty care.
- Thyroidectomy:
For patients with papillary or follicular carcinoma, total thyroidectomy is the recommended treatment of choice. The ATA expert panel recommendation is based on data showing an increased incidence of bilateral (30%) and multifocal (65%) disease.
In patients with a small unilateral tumor confined to the gland, a near-total thyroidectomy-whereby a small amount of thyroid tissue (<1%-2%) is left in place at the entry point of the recurrent laryngeal nerve or superior parathyroid glands-might be considered to decrease permanent damage to those structures.
Total thyroidectomy also optimizes the use of radioactive iodine for imaging and treatment.
- Central neck dissection:
- A therapeutic central neck lymph node dissection should be done in the presence of clinical evidence of central or lateral neck metastases. Larger tumor size (>1 cm), extrathyroidal extension, and multifocal disease are associated with increased risk of nodal metastases.[3]
- For patients with no clinical evidence of gross extrathyroidal invasion or locoregional metastasis, a prophylactic central neck dissection should be considered on the basis of tumor focality and size of the primary tumor. For patients with unifocal disease, ipsilateral central neck dissection, with contralateral central neck dissection based on intraoperative findings, may also be considered.
- Lateral neck dissection:
- Cytological confirmation of metastatic disease to lymph nodes in the lateral neck is recommended before surgery.
- Routine prophylactic lateral neck dissection is not recommended.
- Thyroidectomy:
- Classification and risk assignment.[2]
Despite the limited data in pediatrics, the ATA Task Force recommends the use of the tumor-node-metastasis (TNM) classification system to categorize patients into one of three risk groups. (Refer to the Stage Information for Thyroid Cancer section in the PDQ summary on Thyroid Cancer Treatment [Adult] for more information about the TNM system.) This categorization strategy is meant to define the risk of persistent cervical disease and help determine which patients should undergo postoperative staging for the presence of distant metastasis.
- ATA Pediatric Low Risk: Disease confined to the thyroid with N0 or NX disease or patients with incidental N1a (microscopic metastasis to a small number of central neck nodes). These patients are at lowest risk of distant disease but may still be at risk of residual cervical disease, especially if the initial surgery did not include central neck dissection.
- ATA Pediatric Intermediate Risk: Extensive N1a or minimal N1b disease. These patients are at low risk of distant metastasis but are at an increased risk of incomplete lymph node resection and persistent cervical disease.
- ATA Pediatric High Risk: Regionally extensive disease (N1b) or locally invasive disease (T4), with or without distant metastasis. Patients in this group are at the highest risk of incomplete resection, persistent disease, and distant metastasis.
- Postoperative staging and long-term surveillance.[2]
Initial staging should be performed within 12 weeks after surgery; the purpose is to assess for evidence of persistent locoregional disease and to identify patients who are likely to benefit from additional therapy with iodine I 131 (131I). The ATA Pediatric Risk Level (as defined above) helps determine the extent of postoperative testing.
- ATA Pediatric Low Risk:
- Initial postoperative staging includes a TSH-suppressed thyroglobulin. A diagnostic iodine I 123 (123I) scan is not required.
- TSH suppression should be targeted to serum levels of 0.5 to 1.0 mIU/L.
- In patients with no evidence of disease, surveillance should include ultrasound at 6 months postoperatively and then annually for 5 years; and thyroglobulin levels (on hormone replacement therapy) every 3 to 6 months for 2 years and then annually.
- ATA Pediatric Intermediate Risk:
- Initial postoperative staging includes a TSH-stimulated thyroglobulin and diagnostic 123I whole-body scan for further stratification and determination with 131I.
- TSH suppression should be targeted to serum levels of 0.1 to 0.5 mIU/L.
- In patients with no evidence of disease, surveillance should include ultrasound at 6 months postoperatively and then every 6 to 12 months for 5 years (and then less frequently); and thyroglobulin levels (on hormone replacement therapy) every 3 to 6 months for 3 years and then annually.
- TSH-stimulated thyroglobulin and diagnostic 123I scan should be considered in 1 to 2 years for patients treated with 131I.
- ATA Pediatric High Risk:
- Initial postoperative staging includes a TSH-stimulated thyroglobulin and diagnostic 123I whole-body scan for further stratification and determination with 131I.
- TSH suppression should be targeted to serum levels of less than 0.1 mIU/L.
- In patients with no evidence of disease, surveillance should include ultrasound at 6 months postoperatively and then every 6 to 12 months for 5 years (and then less frequently); and thyroglobulin levels (on hormone replacement therapy) every 3 to 6 months for 3 years and then annually.
- TSH-stimulated thyroglobulin and, possibly, a diagnostic 123I scan in 1 to 2 years in patients treated with 131I.
For patients with anti-thyroglobulin antibodies, consideration can be given to deferred postoperative staging to allow time for antibody clearance, except in patients with T4 or M1 disease.
- ATA Pediatric Low Risk:
- Radioactive iodine ablation.[2]
The goal of 131I therapy is to decrease the risks of recurrence and to decrease mortality by eliminating iodine-avid disease.
- The ATA Task Force recommends the use of 131I for the treatment of iodine-avid persistent locoregional or nodal disease that cannot be resected and known or presumed iodine-avid distant metastases. For patients with persistent disease after administration of 131I, the decision to pursue additional 131I therapy should be individualized on the basis of clinical data and previous response.
- To facilitate 131I uptake by residual iodine-avid disease, the TSH level should be above 30 mIU/L. This level can be achieved by withdrawing levothyroxine for at least 14 days. In patients who cannot mount an adequate TSH response or cannot tolerate profound hypothyroidism, recombinant human TSH may be used.
- Therapeutic 131I administration is commonly based on either empiric dosing or whole-body dosimetry. Based on the lack of data comparing empiric treatment and treatment informed by dosimetry, the ATA Task Force was unable to recommend one specific approach. However, because of the differences in body size and iodine clearance in children compared with adults, it is recommended that all activities of 131I should be calculated by experts with experience in dosing children.
- A posttreatment whole-body scan is recommended for all children 4 to 7 days after 131I therapy. The addition of single-photon emission CT with integrated conventional CT (SPECT/CT) may help to distinguish the anatomic location of focal uptake.
While rare, late effects of 131I treatment include salivary gland dysfunction, bone marrow suppression, pulmonary fibrosis, and second malignancies.[4]
References:
- Waguespack SG, Francis G: Initial management and follow-up of differentiated thyroid cancer in children. J Natl Compr Canc Netw 8 (11): 1289-300, 2010.
- Francis GL, Waguespack SG, Bauer AJ, et al.: Management Guidelines for Children with Thyroid Nodules and Differentiated Thyroid Cancer. Thyroid 25 (7): 716-59, 2015.
- Kim J, Sun Z, Adam MA, et al.: Predictors of nodal metastasis in pediatric differentiated thyroid cancer. J Pediatr Surg 52 (1): 120-123, 2017.
- Albano D, Bertagna F, Panarotto MB, et al.: Early and late adverse effects of radioiodine for pediatric differentiated thyroid cancer. Pediatr Blood Cancer 64 (11): , 2017.
Treatment of Recurrent Papillary and Follicular Thyroid Carcinoma
Patients with differentiated thyroid cancer generally have an excellent survival with relatively few side effects.[1,2,3] However, recurrence is common (35%-45%) and is seen more often in children younger than 10 years and in those with palpable cervical lymph nodes at diagnosis.[4,5] Even patients with a tumor that has spread to the lungs may expect to have no decrease in life span after appropriate treatment.[6] Of note, the sodium-iodide symporter (a membrane-bound glycoprotein cotransporter), essential for uptake of iodide and thyroid hormone synthesis, is expressed in 35% to 45% of thyroid cancers in children and adolescents. Patients with expression of the sodium-iodide symporter have a lower risk of recurrence.[7]
Recurrent papillary thyroid cancer is usually responsive to treatment with radioactive iodine ablation.[8]
Tyrosine kinase inhibitors (TKIs) such as sorafenib have been shown to induce responses in up to 15% of adult patients with metastatic disease.[9] Response to sorafenib has also been documented in a pediatric case.[10]
TKIs approved for the treatment of adults include the following:
- Sorafenib. Sorafenib is a vascular endothelial growth factor receptor (VEGFR), platelet-derived growth factor receptor (PDGFR), and RAS kinase inhibitor. In a randomized phase III trial, sorafenib improved progression-free survival (PFS) when compared with placebo in adult patients with radioactive iodine-refractory locally advanced or metastatic differentiated thyroid cancer.[11] In one case report, sorafenib produced a radiographic response in a patient aged 8 years with metastatic papillary thyroid carcinoma.[12] Sorafenib was approved by the U.S. Food and Drug Administration (FDA) in November 2013 for the treatment of adults with late-stage metastatic differentiated thyroid carcinoma.
- Lenvatinib. Lenvatinib is an oral VEGFR, fibroblast growth factor receptor, PDGFR, RET, and KIT inhibitor. In a phase III randomized study of adults with iodine I 131 (131I)-refractory differentiated thyroid cancer, lenvatinib was associated with a significant improvement in PFS and response rate when compared with a placebo.[13] Lenvatinib was approved by the FDA in February 2015 for the treatment of adults with progressive radioactive iodine-refractory differentiated thyroid carcinoma.
Given the high incidence of BRAF mutations in patients with papillary thyroid carcinoma, the use of selective RAF/MEK inhibitors is being investigated.[9,14,15]
(Refer to the PDQ summary on Thyroid Cancer Treatment [Adult] for more information.)
Treatment Options Under Clinical Evaluation for Recurrent Papillary and Follicular Thyroid Carcinoma
Information about National Cancer Institute (NCI)-supported clinical trials can be found on the NCI website. For information about clinical trials sponsored by other organizations, refer to the ClinicalTrials.gov website.
The following is an example of a national and/or institutional clinical trial that is currently being conducted:
-
APEC1621 (NCT03155620) (Pediatric MATCH: Targeted Therapy Directed by Genetic Testing in Treating Pediatric Patients with Relapsed or Refractory Advanced Solid Tumors, Non-Hodgkin Lymphomas, or Histiocytic Disorders): NCI-COG Pediatric Molecular Analysis for Therapeutic Choice (MATCH), referred to as Pediatric MATCH, will match targeted agents with specific molecular changes identified using a next-generation sequencing targeted assay of more than 3,000 different mutations across more than 160 genes in refractory and recurrent solid tumors. Children and adolescents aged 1 to 21 years are eligible for the trial.
Tumor tissue from progressive or recurrent disease must be available for molecular characterization. Patients with tumors that have molecular variants addressed by treatment arms included in the trial will be offered treatment on Pediatric MATCH. Additional information can be obtained on the ClinicalTrials.gov website for APEC1621 (NCT03155620).
References:
- Vassilopoulou-Sellin R, Goepfert H, Raney B, et al.: Differentiated thyroid cancer in children and adolescents: clinical outcome and mortality after long-term follow-up. Head Neck 20 (6): 549-55, 1998.
- Wiersinga WM: Thyroid cancer in children and adolescents--consequences in later life. J Pediatr Endocrinol Metab 14 (Suppl 5): 1289-96; discussion 1297-8, 2001.
- Jarzab B, Handkiewicz-Junak D, Wloch J: Juvenile differentiated thyroid carcinoma and the role of radioiodine in its treatment: a qualitative review. Endocr Relat Cancer 12 (4): 773-803, 2005.
- Alessandri AJ, Goddard KJ, Blair GK, et al.: Age is the major determinant of recurrence in pediatric differentiated thyroid carcinoma. Med Pediatr Oncol 35 (1): 41-6, 2000.
- Borson-Chazot F, Causeret S, Lifante JC, et al.: Predictive factors for recurrence from a series of 74 children and adolescents with differentiated thyroid cancer. World J Surg 28 (11): 1088-92, 2004.
- Biko J, Reiners C, Kreissl MC, et al.: Favourable course of disease after incomplete remission on (131)I therapy in children with pulmonary metastases of papillary thyroid carcinoma: 10 years follow-up. Eur J Nucl Med Mol Imaging 38 (4): 651-5, 2011.
- Patel A, Jhiang S, Dogra S, et al.: Differentiated thyroid carcinoma that express sodium-iodide symporter have a lower risk of recurrence for children and adolescents. Pediatr Res 52 (5): 737-44, 2002.
- Powers PA, Dinauer CA, Tuttle RM, et al.: Treatment of recurrent papillary thyroid carcinoma in children and adolescents. J Pediatr Endocrinol Metab 16 (7): 1033-40, 2003.
- Kloos RT, Ringel MD, Knopp MV, et al.: Phase II trial of sorafenib in metastatic thyroid cancer. J Clin Oncol 27 (10): 1675-84, 2009.
- Waguespack SG, Sherman SI, Williams MD, et al.: The successful use of sorafenib to treat pediatric papillary thyroid carcinoma. Thyroid 19 (4): 407-12, 2009.
- Brose MS, Nutting CM, Jarzab B, et al.: Sorafenib in radioactive iodine-refractory, locally advanced or metastatic differentiated thyroid cancer: a randomised, double-blind, phase 3 trial. Lancet 384 (9940): 319-28, 2014.
- Iyer P, Mayer JL, Ewig JM: Response to sorafenib in a pediatric patient with papillary thyroid carcinoma with diffuse nodular pulmonary disease requiring mechanical ventilation. Thyroid 24 (1): 169-74, 2014.
- Schlumberger M, Tahara M, Wirth LJ, et al.: Lenvatinib versus placebo in radioiodine-refractory thyroid cancer. N Engl J Med 372 (7): 621-30, 2015.
- Falchook GS, Long GV, Kurzrock R, et al.: Dabrafenib in patients with melanoma, untreated brain metastases, and other solid tumours: a phase 1 dose-escalation trial. Lancet 379 (9829): 1893-901, 2012.
- Hayes DN, Lucas AS, Tanvetyanon T, et al.: Phase II efficacy and pharmacogenomic study of Selumetinib (AZD6244; ARRY-142886) in iodine-131 refractory papillary thyroid carcinoma with or without follicular elements. Clin Cancer Res 18 (7): 2056-65, 2012.
Treatment of Medullary Thyroid Carcinoma
Medullary thyroid carcinomas are commonly associated with the multiple endocrine neoplasia 2 (MEN2) syndrome (refer to the Multiple Endocrine Neoplasia [MEN] Syndromes and Carney Complex section of the PDQ summary on Unusual Cancers of Childhood Treatment for more information). They present with a more aggressive clinical course; 50% of the cases have hematogenous metastases at diagnosis.[1] Patients with medullary carcinoma of the thyroid have a guarded prognosis, unless they have very small tumors (microcarcinoma, defined as <1.0 cm in diameter), which carry a good prognosis.[2] A natural history study of children and young adults with medullary thyroid cancer is being conducted by the National Cancer Institute (NCT01660984). For patients with de novo RET mutations and no familial history, nonendocrine manifestations, such as intestinal ganglioneuromatosis or skeletal or ocular stigmata, may facilitate early diagnosis and result in better outcomes.[3]
Treatment options for medullary thyroid carcinoma include the following:
-
Surgery: Treatment for children with medullary thyroid carcinoma is mainly surgical. A review of 430 patients aged 0 to 21 years with medullary thyroid cancer reported that older age (16-21 years) at diagnosis, tumor diameter greater than 2 cm, positive margins after total thyroidectomy, and lymph node metastases were associated with a worse prognosis.[4] This suggests that central neck node dissection and dissection of nearby positive nodes should improve the 10-year survival for these patients.
Most cases of medullary thyroid carcinoma occur in the context of the MEN2A and MEN2B syndromes. In those familial cases, early genetic testing and counseling is indicated, and prophylactic surgery is recommended for children with the RET germline mutation. Strong genotype-phenotype correlations have facilitated the development of guidelines for intervention, including screening and age at which prophylactic thyroidectomy should occur.[1]
-
Tyrosine kinase inhibitor (TKI) therapy: A number of TKIs have been evaluated and approved for patients with advanced thyroid carcinoma.
- Vandetanib. Vandetanib (an inhibitor of RET kinase, vascular endothelial growth factor receptor [VEGFR], and epidermal growth factor receptor signaling) is approved by the U.S. Food and Drug Administration (FDA) for the treatment of symptomatic or progressive medullary thyroid cancer in adult patients with unresectable, locally advanced, or metastatic disease. Approval was based on a randomized, placebo-controlled, phase III trial that showed a marked progression-free survival improvement for patients randomly assigned to receive vandetanib (hazard ratio, 0.35); the trial also showed an objective response rate advantage for patients receiving vandetanib (44% vs. 1% for the placebo arm).[5,6]
Children with locally advanced or metastatic medullary thyroid carcinoma were treated with vandetanib in a phase I/II trial. Of 16 patients, only 1 had no response, and 7 had a partial response, for an objective response rate of 44%. Disease in three of those patients subsequently recurred, but 11 of 16 patients treated with vandetanib remained on therapy at the time of the report. The median duration of therapy for the entire cohort was 27 months, with a range of 2 to 52 months.[7]
- Cabozantinib. Cabozantinib (an inhibitor of the RET and MET kinases and VEGFR) has also shown activity against unresectable medullary thyroid cancer (10 of 35 adult patients [29%] had a partial response).[8] Cabozantinib was approved by the FDA in November 2012 for the treatment of adults with metastatic medullary thyroid cancer.
- Vandetanib. Vandetanib (an inhibitor of RET kinase, vascular endothelial growth factor receptor [VEGFR], and epidermal growth factor receptor signaling) is approved by the U.S. Food and Drug Administration (FDA) for the treatment of symptomatic or progressive medullary thyroid cancer in adult patients with unresectable, locally advanced, or metastatic disease. Approval was based on a randomized, placebo-controlled, phase III trial that showed a marked progression-free survival improvement for patients randomly assigned to receive vandetanib (hazard ratio, 0.35); the trial also showed an objective response rate advantage for patients receiving vandetanib (44% vs. 1% for the placebo arm).[5,6]
(Refer to the Multiple Endocrine Neoplasia [MEN] Syndromes and Carney Complex section of the PDQ summary on Unusual Cancers of Childhood Treatment and the Treatment for those with MTC section in the PDQ summary on Genetics of Endocrine and Neuroendocrine Neoplasias for more information.)
Treatment Options Under Clinical Evaluation for Medullary Thyroid Carcinoma
Information about National Cancer Institute (NCI)-supported clinical trials can be found on the NCI website. For information about clinical trials sponsored by other organizations, refer to the ClinicalTrials.gov website.
The following is an example of a national and/or institutional clinical trial that is currently being conducted:
-
APEC1621 (NCT03155620) (Pediatric MATCH: Targeted Therapy Directed by Genetic Testing in Treating Pediatric Patients with Relapsed or Refractory Advanced Solid Tumors, Non-Hodgkin Lymphomas, or Histiocytic Disorders): NCI-COG Pediatric Molecular Analysis for Therapeutic Choice (MATCH), referred to as Pediatric MATCH, will match targeted agents with specific molecular changes identified using a next-generation sequencing targeted assay of more than 3,000 different mutations across more than 160 genes in refractory and recurrent solid tumors. Children and adolescents aged 1 to 21 years are eligible for the trial.
Tumor tissue from progressive or recurrent disease must be available for molecular characterization. Patients with tumors that have molecular variants addressed by treatment arms included in the trial will be offered treatment on Pediatric MATCH. Additional information can be obtained on the ClinicalTrials.gov website for APEC1621 (NCT03155620).
References:
- Waguespack SG, Rich TA, Perrier ND, et al.: Management of medullary thyroid carcinoma and MEN2 syndromes in childhood. Nat Rev Endocrinol 7 (10): 596-607, 2011.
- Krueger JE, Maitra A, Albores-Saavedra J: Inherited medullary microcarcinoma of the thyroid: a study of 11 cases. Am J Surg Pathol 24 (6): 853-8, 2000.
- Brauckhoff M, Machens A, Lorenz K, et al.: Surgical curability of medullary thyroid cancer in multiple endocrine neoplasia 2B: a changing perspective. Ann Surg 259 (4): 800-6, 2014.
- Raval MV, Sturgeon C, Bentrem DJ, et al.: Influence of lymph node metastases on survival in pediatric medullary thyroid cancer. J Pediatr Surg 45 (10): 1947-54, 2010.
- Wells SA Jr, Robinson BG, Gagel RF, et al.: Vandetanib in patients with locally advanced or metastatic medullary thyroid cancer: a randomized, double-blind phase III trial. J Clin Oncol 30 (2): 134-41, 2012.
- Thornton K, Kim G, Maher VE, et al.: Vandetanib for the treatment of symptomatic or progressive medullary thyroid cancer in patients with unresectable locally advanced or metastatic disease: U.S. Food and Drug Administration drug approval summary. Clin Cancer Res 18 (14): 3722-30, 2012.
- Fox E, Widemann BC, Chuk MK, et al.: Vandetanib in children and adolescents with multiple endocrine neoplasia type 2B associated medullary thyroid carcinoma. Clin Cancer Res 19 (15): 4239-48, 2013.
- Kurzrock R, Sherman SI, Ball DW, et al.: Activity of XL184 (Cabozantinib), an oral tyrosine kinase inhibitor, in patients with medullary thyroid cancer. J Clin Oncol 29 (19): 2660-6, 2011.
Special Considerations for the Treatment of Children With Cancer
Cancer in children and adolescents is rare, although the overall incidence of childhood cancer has been slowly increasing since 1975.[1] Referral to medical centers with multidisciplinary teams of cancer specialists experienced in treating cancers that occur in childhood and adolescence should be considered for children and adolescents with cancer. This multidisciplinary team approach incorporates the skills of the following health care professionals and others to ensure that children receive treatment, supportive care, and rehabilitation that will achieve optimal survival and quality of life:
- Primary care physicians.
- Pediatric surgeons.
- Radiation oncologists.
- Pediatric medical oncologists/hematologists.
- Rehabilitation specialists.
- Pediatric nurse specialists.
- Social workers.
- Child-life professionals.
- Psychologists.
(Refer to the PDQ Supportive and Palliative Care summaries for specific information about supportive care for children and adolescents with cancer.)
Guidelines for pediatric cancer centers and their role in the treatment of pediatric patients with cancer have been outlined by the American Academy of Pediatrics.[2] At these pediatric cancer centers, clinical trials are available for most types of cancer that occur in children and adolescents, and the opportunity to participate in these trials is offered to most patients and their families. Clinical trials for children and adolescents diagnosed with cancer are generally designed to compare potentially better therapy with therapy that is currently accepted as standard. Most of the progress made in identifying curative therapy for childhood cancers has been achieved through clinical trials. Information about ongoing clinical trials is available from the NCI website.
Dramatic improvements in survival have been achieved for children and adolescents with cancer. Between 1975 and 2010, childhood cancer mortality decreased by more than 50%.[3] Childhood and adolescent cancer survivors require close monitoring because cancer therapy side effects may persist or develop months or years after treatment. (Refer to the PDQ summary on Late Effects of Treatment for Childhood Cancer for specific information about the incidence, type, and monitoring of late effects in childhood and adolescent cancer survivors.)
Childhood cancer is a rare disease, with about 15,000 cases diagnosed annually in the United States in individuals younger than 20 years.[4] The U.S. Rare Diseases Act of 2002 defines a rare disease as one that affects populations smaller than 200,000 persons and, by definition, all pediatric cancers are considered rare. The designation of a pediatric rare tumor is not uniform among international groups, as follows:
- The Italian Rare Tumors in Pediatric Age (TREP) cooperative project defines a pediatric rare tumor as one with an incidence of less than two cases per 1 million population per year and is not included in other clinical trials.[5]
- The Children's Oncology Group has opted to define rare pediatric cancers as those listed in the International Classification of Childhood Cancer subgroup XI, which includes thyroid cancer, melanoma and nonmelanoma skin cancers, and multiple types of carcinomas (e.g., adrenocortical carcinoma, nasopharyngeal carcinoma, and most adult-type carcinomas such as breast cancer, colorectal cancer, etc.).[6] These diagnoses account for about 4% of cancers diagnosed in children aged 0 to 14 years, compared with about 20% of cancers diagnosed in adolescents aged 15 to 19 years.[7] Most cancers within subgroup XI are either melanomas or thyroid cancer, with the remaining subgroup XI cancer types accounting for only 1.3% of cancers in children aged 0 to 14 years and 5.3% of cancers in adolescents aged 15 to 19 years.
These rare cancers are extremely challenging to study because of the low incidence of patients with any individual diagnosis, the predominance of rare cancers in the adolescent population, and the lack of clinical trials for adolescents with rare cancers.
Information about these tumors may also be found in sources relevant to adults with cancer such as the PDQ summary on Thyroid Cancer Treatment (Adult).
References:
- Smith MA, Seibel NL, Altekruse SF, et al.: Outcomes for children and adolescents with cancer: challenges for the twenty-first century. J Clin Oncol 28 (15): 2625-34, 2010.
- Corrigan JJ, Feig SA; American Academy of Pediatrics: Guidelines for pediatric cancer centers. Pediatrics 113 (6): 1833-5, 2004.
- Smith MA, Altekruse SF, Adamson PC, et al.: Declining childhood and adolescent cancer mortality. Cancer 120 (16): 2497-506, 2014.
- Ward E, DeSantis C, Robbins A, et al.: Childhood and adolescent cancer statistics, 2014. CA Cancer J Clin 64 (2): 83-103, 2014 Mar-Apr.
- Ferrari A, Bisogno G, De Salvo GL, et al.: The challenge of very rare tumours in childhood: the Italian TREP project. Eur J Cancer 43 (4): 654-9, 2007.
- Pappo AS, Krailo M, Chen Z, et al.: Infrequent tumor initiative of the Children's Oncology Group: initial lessons learned and their impact on future plans. J Clin Oncol 28 (33): 5011-6, 2010.
- Howlader N, Noone AM, Krapcho M, et al., eds.: SEER Cancer Statistics Review, 1975-2012. Bethesda, Md: National Cancer Institute, 2015. Also available online. Last accessed November 30, 2017.
Changes to This Summary (02 / 02 / 2018)
The PDQ cancer information summaries are reviewed regularly and updated as new information becomes available. This section describes the latest changes made to this summary as of the date above.
Clinical Presentation and Outcome
Added Al-Qurayshi et al. as reference 6.
This summary is written and maintained by the PDQ Pediatric Treatment Editorial Board, which is editorially independent of NCI. The summary reflects an independent review of the literature and does not represent a policy statement of NCI or NIH. More information about summary policies and the role of the PDQ Editorial Boards in maintaining the PDQ summaries can be found on the About This PDQ Summary and PDQ® - NCI's Comprehensive Cancer Database pages.
About This PDQ Summary
Purpose of This Summary
This PDQ cancer information summary for health professionals provides comprehensive, peer-reviewed, evidence-based information about the treatment of childhood thyroid cancer. It is intended as a resource to inform and assist clinicians who care for cancer patients. It does not provide formal guidelines or recommendations for making health care decisions.
Reviewers and Updates
This summary is reviewed regularly and updated as necessary by the PDQ Pediatric Treatment Editorial Board, which is editorially independent of the National Cancer Institute (NCI). The summary reflects an independent review of the literature and does not represent a policy statement of NCI or the National Institutes of Health (NIH).
Board members review recently published articles each month to determine whether an article should:
- be discussed at a meeting,
- be cited with text, or
- replace or update an existing article that is already cited.
Changes to the summaries are made through a consensus process in which Board members evaluate the strength of the evidence in the published articles and determine how the article should be included in the summary.
The lead reviewers for Childhood Thyroid Cancer Treatment are:
- Denise Adams, MD (Children's Hospital Boston)
- Karen J. Marcus, MD (Dana-Farber Cancer Institute/Boston Children's Hospital)
- Paul A. Meyers, MD (Memorial Sloan-Kettering Cancer Center)
- Thomas A. Olson, MD (Aflac Cancer and Blood Disorders Center of Children's Healthcare of Atlanta - Egleston Campus)
- Alberto S. Pappo, MD (St. Jude Children's Research Hospital)
- R Beverly Raney, MD (Consultant)
- Arthur Kim Ritchey, MD (Children's Hospital of Pittsburgh of UPMC)
- Carlos Rodriguez-Galindo, MD (St. Jude Children's Research Hospital)
- Stephen J. Shochat, MD (St. Jude Children's Research Hospital)
Any comments or questions about the summary content should be submitted to Cancer.gov through the NCI website's Email Us. Do not contact the individual Board Members with questions or comments about the summaries. Board members will not respond to individual inquiries.
Levels of Evidence
Some of the reference citations in this summary are accompanied by a level-of-evidence designation. These designations are intended to help readers assess the strength of the evidence supporting the use of specific interventions or approaches. The PDQ Pediatric Treatment Editorial Board uses a formal evidence ranking system in developing its level-of-evidence designations.
Permission to Use This Summary
PDQ is a registered trademark. Although the content of PDQ documents can be used freely as text, it cannot be identified as an NCI PDQ cancer information summary unless it is presented in its entirety and is regularly updated. However, an author would be permitted to write a sentence such as "NCI's PDQ cancer information summary about breast cancer prevention states the risks succinctly: [include excerpt from the summary]."
The preferred citation for this PDQ summary is:
PDQ® Pediatric Treatment Editorial Board. PDQ Childhood Thyroid Cancer Treatment. Bethesda, MD: National Cancer Institute. Updated <MM/DD/YYYY>. Available at: https://www.cancer.gov/types/thyroid/hp/child-thyroid-treatment-pdq. Accessed <MM/DD/YYYY>. [PMID: 26389315]
Images in this summary are used with permission of the author(s), artist, and/or publisher for use within the PDQ summaries only. Permission to use images outside the context of PDQ information must be obtained from the owner(s) and cannot be granted by the National Cancer Institute. Information about using the illustrations in this summary, along with many other cancer-related images, is available in Visuals Online, a collection of over 2,000 scientific images.
Disclaimer
Based on the strength of the available evidence, treatment options may be described as either "standard" or "under clinical evaluation." These classifications should not be used as a basis for insurance reimbursement determinations. More information on insurance coverage is available on Cancer.gov on the Managing Cancer Care page.
Contact Us
More information about contacting us or receiving help with the Cancer.gov website can be found on our Contact Us for Help page. Questions can also be submitted to Cancer.gov through the website's Email Us.
Last Revised: 2018-02-02